The first and only FDA-approved unrelated cell therapy for hematologic transplant
Give patients with hematologic malignancies and severe aplastic anemia a readily available treatment option15
Give patients with hematologic malignancies and severe aplastic anemia a readily available treatment option15
Today's transplant landscape
Allo-HCT has curative potential, but no new donor sources have been introduced to overcome the challenges of availability, suitability, and deliverability
Availability
of an HLA-matched donor
SUITABILITY
of the donor source that minimizes the risk of post-transplant complications
DELIVERABILITY
of a donor source that sets consistent expectations for time to transplant
Appropriately HLA-matched donors are preferred for allo-HCT, but are not available for all patients
Matched related donors are only available for
30% of patients1
30% of patients1
Matched unrelated donor availability varies greatly, and racially and ethnically diverse donors are underrepresented in donor registries2

79%
White patients of European descent

60%
Native American patients

48%
Hispanic or Latino patients

47%
Asian or Pacific Islander patients
29%
Black or African American patients
There is
no universal
standard of care
no universal
standard of care
Alternative Donor Sources

- Haploidentical
- Mismatched unrelated
- Umbilical cord blood
Potential Risks3,4,5,6

Although alternative donor sources provide more options for patients, there may be additional risks associated, such as higher rates of graft-versus-host-disease (GvHD), infections, and non-relapse mortality (NRM).
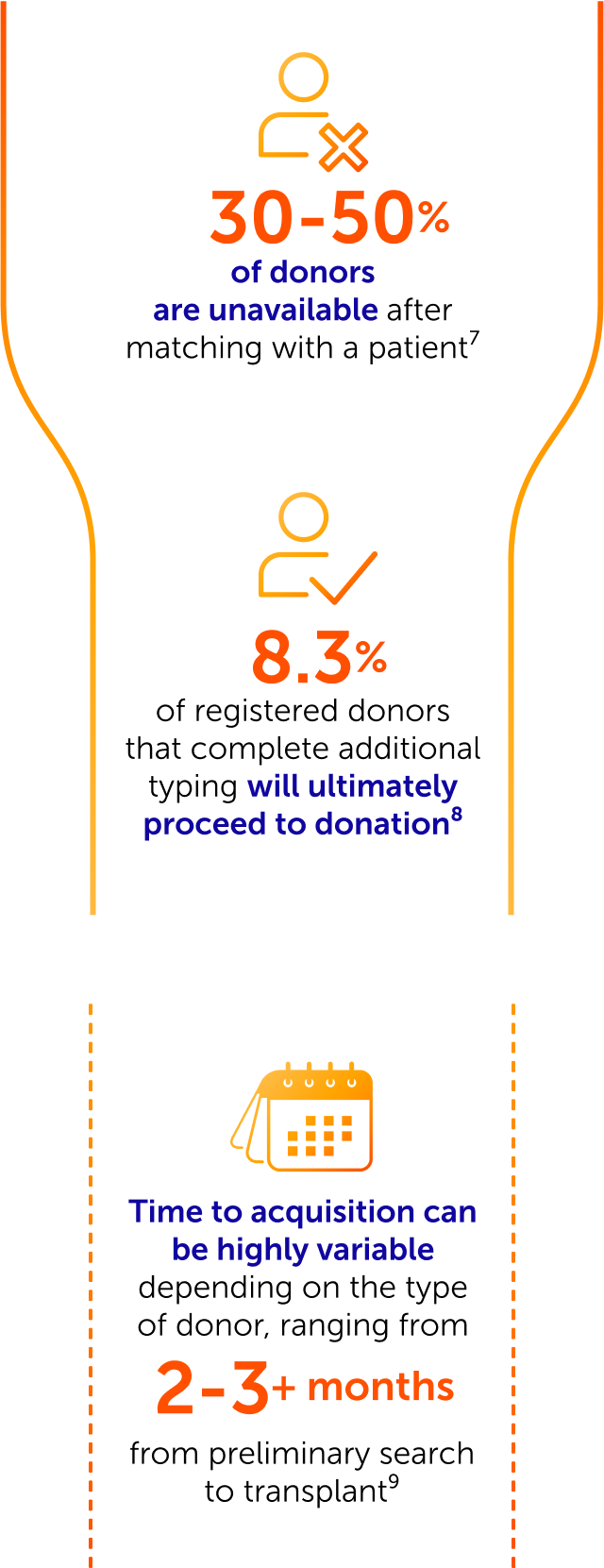
Deliverability factors, including unrelated matched donor attrition and acquisition challenges may delay or prevent a patient from receiving an allo-HCT

Start your patient’s Omisirge treatment journey today




Find an Omisirge treatment center near you
Omisirge is available at transplant centers nationwide. Find an Omisirge transplant center near your patient.